Discharging a patient with amyotrophic lateral sclerosis (ALS) and respiratory involvement is not a routine transition.
In most post-acute scenarios, patients stabilize, receive equipment, and gradually return toward baseline. ALS follows a different path. Patients go home with a progressive condition, increasing respiratory needs, and caregivers who must quickly learn to manage complex ventilation support in real time.
For hospital teams, this moment carries weight. It marks a critical transition in the care journey, where the quality of support at home can significantly influence outcomes.
Respiratory failure remains the leading cause of death in ALS, and the transition from hospital to home is a key inflection point. Early, well-coordinated ventilation support can improve both quality of life and survival, while delayed or poorly managed noninvasive ventilation (NIV) is associated with worse outcomes.1
For discharge planners, case managers, and ALS clinics, choosing a DME partner is not simply operational. It is a clinical decision that shapes what happens next.
Why ALS Requires a Different Post-Acute Approach
ALS is a progressive neurodegenerative disease that affects both upper and lower motor neurons. Respiratory muscle weakness is not a late-stage issue, rather it is central to the disease from early on.
Most patients will require noninvasive ventilation (NIV) during the course of their disease, often earlier than traditional thresholds suggest.
- Declines in inspiratory strength may occur before FVC drops below 50%
- Waiting for traditional thresholds may delay therapy initiation2
Unlike other respiratory populations:
- ALS patients do not stabilize after discharge
- They progress into greater dependence on ventilation
- Their needs require continuous reassessment and adjustment
This creates a fundamentally different care model, one that standard DME approaches are not designed to support.

How ALS Care Differs from Standard DME Models
ALS respiratory care requires a longitudinal, clinically integrated approach, not a transactional one.
| Dimension | Standard Post‑Acute DME | ALS Respiratory Care |
|---|---|---|
| Timeline | Weeks to months; patient stabilizes or recovers | Months to years; patient progresses into greater dependence |
| Equipment trajectory | Static or decreasing needs over time | Escalating needs; settings and interfaces require ongoing adjustment |
| Reassessment frequency | Periodic or as‑needed | Continuous; respiratory status changes unpredictably |
| Caregiver involvement | Variable; often supplemental | Central; caregivers manage daily therapy and troubleshooting |
| Clinical coordination | Primarily with referring physician | Multidisciplinary coordination across neurology, pulmonology, respiratory therapy, palliative care, and community services |
| DME relationship model | Transactional; equipment delivery and periodic resupply | Longitudinal; ongoing clinical relationship with proactive support |
This distinction directly shapes what patients, caregivers, and clinical teams need from a home medical equipment partner.
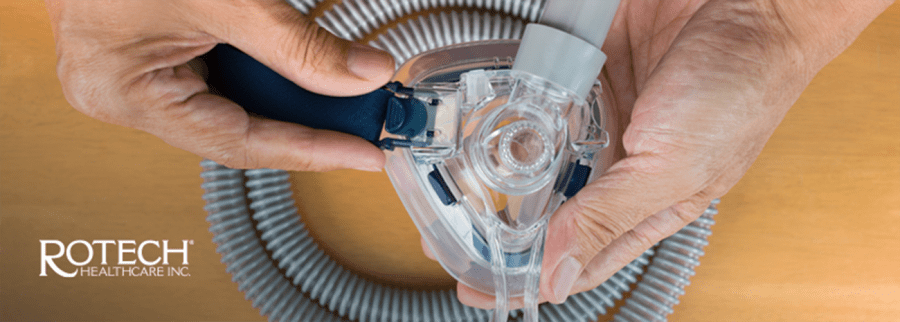
Ventilation in ALS: More Than Supplying a Device
Noninvasive ventilation (NIV) has been shown to improve survival and quality of life in ALS patients with respiratory insufficiency.3
But outcomes depend on how therapy is implemented, not just whether it is prescribed.
Effective ALS ventilation requires:
- proper patient acclimation
- interface optimization
- ongoing setting adjustments
- early troubleshooting of tolerance issues
Common barriers include:
- mask discomfort
- air leaks
- pressure intolerance
- disrupted sleep
Without early intervention, patients may abandon therapy.
Education is equally critical. Patients and caregivers must understand:
- how the equipment works
- what to expect during adaptation
- when to seek help
Studies show adherence improves significantly with structured education and ongoing support.4
See How We Support ALS Patients

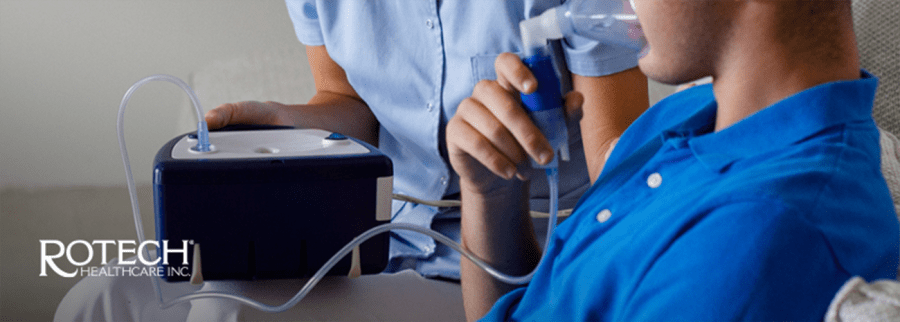
The Caregiver Factor in ALS Ventilation
Caregivers are central to ALS respiratory care.
They manage:
- daily ventilation therapy
- equipment troubleshooting
- nighttime monitoring
- escalation of concerns
Research shows caregiver burden increases significantly once ventilation is required, with some providing up to 14 hours of care per day.5
Such demands lead nearly 30% of caregivers to report that their own quality of life is worse than the patient’s.5 Caregiver strain directly impacts patient outcomes, in addition to quality of life. Supporting caregivers is a core component of effective ALS care.
What Hospitals Should Expect from a DME Partner
Not all DME providers are equipped to support ALS patients. Hospital teams should look for partners with capabilities aligned to the complexity of the disease.
1. Disease-Specific Clinical Expertise
DME partner should have respiratory therapists and clinicians with direct experience managing neuromuscular disease — staff who understand the progression trajectory, the interface challenges, and the need for ongoing adjustment.
2. A Single Point of Contact for Coordination
The DME partner should provide a dedicated contact, so someone who knows the patient, can liaise with the ALS clinic and pulmonology team, and can expedite responses when needs change.
3. Capacity for Longitudinal Support
The partner should have systems in place for ongoing monitoring, periodic reassessment, and proactive outreach, not just reactive service when patients call with problems.
4. Responsiveness to Changing Needs
When a patient’s respiratory status declines, the DME partner must be able to respond quickly, adjusting settings, changing interfaces, or escalating support without lengthy approval delays.
5. Comfort Managing Complex Ventilator Therapy
This includes not just standard bilevel devices, but portable home ventilators, volume-targeted modes, and coordination with airway clearance strategies. The partner should be able to manage the full spectrum of respiratory support that ALS patients may eventually require.
6. Caregiver Education and Support
Caregivers are the frontline of home ventilation in ALS. The DME partner should provide structured training, accessible resources, and ongoing availability for questions and troubleshooting.

Inside Rotech’s ALS Ventilation Program
Rotech Healthcare’s ALS Ventilation Program is designed to support patients, caregivers, and clinical teams throughout the progression of the disease. The program functions as an extension of the care team in the home.
Key features include:
- Individualized plans of care tailored to disease stage and patient needs
- Dedicated Ventilator Patient Specialist serving as a single point of contact
- Patient and caregiver education for confidence and adherence
- Ongoing in-home visits and follow-up
- Coordination with ALS clinics and physicians
- Continuous titration of settings per physician orders
- Spirometry and FVC monitoring
- Portable ventilators to support mobility and independence
- Backup ventilator options when appropriate
- 24/7 clinical support for real-time troubleshooting
This model supports both clinical continuity and patient stability outside the hospital.
Key Takeaways for Discharge Teams
For hospital teams managing ALS patients with respiratory involvement:
- Engage DME partners early
Ideally at the time of NIV consideration, not during crisis - Prioritize ALS-specific expertise
Not all respiratory providers have neuromuscular experience - Ensure clear communication pathways
Coordination gaps create care gaps - Assess caregiver readiness
Education and support reduce downstream complications - Plan for progression
ALS care is long-term — choose partners who can adapt over time
Frequently Asked Questions About NIV
Why is ALS ventilation different from COPD?
ALS involves progressive muscle weakness, requiring continuous adjustment and caregiver involvement.
When should ALS patients start noninvasive ventilation?
Earlier initiation may improve outcomes. Waiting for traditional thresholds like FVC <50% may delay benefit.2
How often should ventilator settings be adjusted?
Regular reassessment is expected as respiratory function declines.
Why is caregiver support critical?
Caregivers manage daily therapy. Their ability to do so directly impacts adherence and outcomes.

Conclusion
ALS post-acute care, particularly for patients with respiratory involvement, requires a different approach than standard DME models provide.
The progressive nature of the disease, the centrality of respiratory support, the burden on caregivers, and the need for ongoing coordination all demand partners who understand ALS as a long-term clinical relationship, not a one-time equipment delivery.
For hospital teams and ALS clinics, the choice of DME partner is a meaningful clinical decision. The right partnership reduces friction, supports patients through transitions, and aligns post-acute care with the goals established by the care team.
Rotech’s ALS Ventilation Program was built with these principles in mind, not as a product, but as a model of care designed to extend the reach of clinical teams into the home setting where ALS patients spend most of their lives.
Learn More About Rotech’s ALS Program
References
- Zimnoch, M., Eldeiry, D., Oluwabunmi Aruleba, Schwartz, J., Avaricio, M., Ishikawa, O., Mina, B., & Esquinas, A. (2025). Non-Invasive Ventilation: When, Where, How to Start, and How to Stop. Journal of Clinical Medicine, 14(14), 5033–5033. https://doi.org/10.3390/jcm14145033
- Jimenez, J. V., Tang, M. J., Wilson, M. W., Morrison, A. H., Ackrivo, J., & Choi, P. J. (2024). Initiation of noninvasive ventilation in patients with amyotrophic lateral sclerosis. Muscle & Nerve, 70(5), 1099–1103. https://doi.org/10.1002/mus.28250
- Sancho, J., Ferrer, S., & Signes-Costa, J. (2025). Noninvasive Ventilation Effectiveness in Amyotrophic Lateral Sclerosis. Journal of Clinical Medicine, 14(23), 8609. https://doi.org/10.3390/jcm14238609
- Sau, D., Li, P. W.-C., Lau, J. C.-C., Alice, S., Ip, M., Linda, L., Chung, H., & Iris, K. (2024). Health Communication and Adherence to Noninvasive Ventilation in Chronic Hypercapnic Respiratory Failure. JAMA Network Open, 7(12), e2451614–e2451614. https://doi.org/10.1001/jamanetworkopen.2024.51614
- Tang, S., Li, L., Xue, H., Cao, S., Li, C., Han, K., & Wang, B. (2021). Caregiver burden and associated factors among primary caregivers of patients with ALS in home care: a cross-sectional survey study. BMJ Open, 11(9), e050185. https://doi.org/10.1136/bmjopen-2021-050185